1.1 Hemodynamics: Basic Principles for Anesthesiology and Intensive Medicine
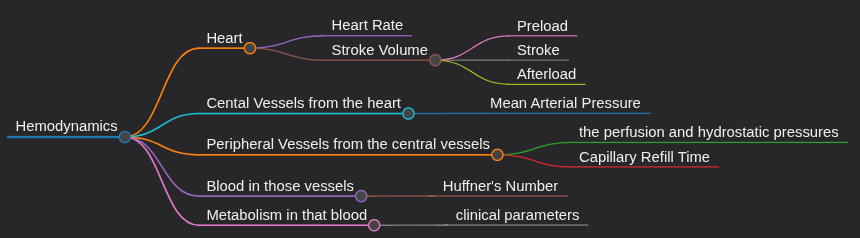
Okay, so the hemodynamics have 5 main parts:
- The heart (obviously)
- The central vessels coming out of the heart
- The peripheral vessels coming from the central ones
- The Blood in those vessels
- The metabolism in that blood
The heart
The concept in the heart section is Cardiodynamics.
Now, first of all, we have the heart. It is a pump that circulates blood around our body. This parameter can be defined as the Cardiac Output (CO). CO depends on the heart rate (ie. how many times the heart beats per minute) and the Stroke Volume (which is how much blood in milliliters does the heart pump in each beat). Our average heart rate is around 70 beats/min and the average stroke volume is 80 ml. If we multiply them we get 5.6 liters per minute which means that our heart pumps our entire blood volume through our body each minute.
Lets take a look at each of these factors (heart rate and stroke volume) more closely. First is heart rate; it is easy. It can be influenced by physical activity, autonomic nervous system etc.
Stroke volume is tricky. We can think of this like the heart is a pump right. The blood first has to come into the heart, the heart has to pump that blood out but also, some blood might remain in the heart even after the beat. The blood coming into the heart is the preload, The beat is the stroke and some blood that remains inside at the end is the afterload.
- Preload
This is the blood that comes into the ventricles to get pumped. But where does it come from? It comes from the atria. Also, let us quickly define systole and diastole. Systole is when blood is pumped from the ventricles to the body and diastole is when the artia contract to send the blood into the ventricles. So essentially, preload is what is in the ventricles after the diastole (after the atria have contracted) which is why it is also called End-Diastolic Volume (EDV).
We can estimate preloads for both the right and left ventricles. For right ventricle, we can look at where the blood is coming from. From the atria. And where are they getting the blood from? The central veins. So Central Venous Pressure can give us an estimate for the pressure in the right ventricle. Central Venous pressure reference value is around 2 to 10 mmHg; its very low. For the left ventricle, where does the blood come from? The left atrium. The reference value for left atrial pressure is around 10 to 12 mmHg. They can be memorized by just remembering that one is 2 - 10 and the other is 10 to 12.
- Stroke Volume
This the actual beat of the heart. Now which factors might be able to influence this? Its actually pretty unique. The heart doesn't really need the brain to tell it that we are doing physical exercice and you need to pump harder and faster. What??
Yes, actually the preload can determine the strength of the contraction of the heart. The higher the preload, the harder the heart pumps the blood and greater the stroke volume. Now, how does this happen? Actually, the more blood that comes into the ventricles, the more stretched they are. This does two things:
- It stretches the myocardial muscle which allows them to generate more force.
- It increases the sensitivity of Troponin C to Ca2+
Now what is the clinical parameter for Stroke Volume? Contractility. It is the pressure developed in the ventricles during the time in which they are pumping (so pressure developed during the systole divided by the systolic time).
- After load
It is the tension in the heart muscle after the beat; at the end of the systole (End Systolic Volume).
The global parameter for heart function that merges all of these into one is the Ejection Fraction (EF). It is usually around 66%. It is calculated by dividing the Stroke volume (which was 80 ml) by End Diastolic Volume (which is the blood that remains in the left ventricle after the atria contract - so the ventricles are full of blood now; which is 120 ml). So we are essentially saying what percentage of the blood that comes into the ventricle (120 ml) is being pumped out (80 ml)? 66%.
The Central Vessels
The central vessel from the heart directly is the aorta. The clinical parameter we can check is the pressure in it (of course). This is expressed in the Mean Arterial Pressure (MAP). The formula is simple:
MAP = Diastolic pressure + 1/3 (Systolic - Diastolic Pressure)
which equates to around 75 to 100 mmHg. The normal Systolic value range is 120 - 140 and Diastolic value is 80 mmHg.
Now, the other important value is how much pressure is being used to push nutrients from the blood into the tissue space. In my opinion, this should under the peripheral vessels heading but okay. This is known as the perfusion pressure. It is defined by the pressure being sent in the aorta and the pressure remaining in the central veins coming back to the heart so pressure in the aorta (MAP) - pressure back in the central veins (CVP). This can be calculated as 80 - 5 which is 75 mmHg of perfusion pressure.
The Peripheral Circulation
The volume flow depends on two factors of the vessel environment. The pressure trying to push fluid out of the capillaries and the pressure trying to pull fluid back in. The pressure trying to push fluids out is the perfusion pressure and the pressure trying to pull everything back inside is the oncotic pressure. Perfusion pressure is easy to understand now. Oncotic pressure exists because of hydrostatic forces of the proteins of the blood. Water wants to stay close to the proteins so it is being pulled back into the vessels.
Now, the other factor we can easily see in the peripheral circulation is Capillary Refill Time. It should be less than 2 seconds when we press on the skin and it turns from white back to red/skin color. In states of shock (eg. in case of a lot of blood loss), the capillary refill time will increase to 3 or 4 seconds or even more. The other parameter to check in peripheral circulation is the difference between core body temperature and the peripheral one. If it is more than 5 degrees, then there is low circulation there.
The Blood
The important fact to remember here is the Huffner's number which is 1.34 ml of Oxygen carried by 1 gram of Hemoglobin.
The Metabolism
The metabolism can be generally estimated by checking the pH of the blood. If it is less than 7.34, there is increased lactic acid in serum and the partial pressures of Oxygen and Carbon Dioxide are low then metabolism is not in homeostatis.